
Forecasting the CY 2027 Medicare PFS Proposed Rule
It’s that time of year again as we anticipate the Centers for Medicare and Medicaid Services (CMS) release of the CY 2027 Medicare Physician Fee Schedule (PFS) Proposed Rule. It is usually published around July 1, but last year it wasn’t released until July 14, which was unusually late for a rule release. While it is unclear whether this year’s rule will be released before the 4th of July holiday, there is no indication that the 2027 Proposed Rule will be delayed as much as last year’s rule was.
Insights from the 2026 Medicare PFS, recent CMS initiatives, and public comments from CMS leadership offer guidance on what to expect in the 2027 Medicare PFS Proposed Rule. Five key themes to watch for are outlined below.
#1: Growing Disparity Between Dual Conversion Factors.
Clinicians participating in advanced payment models are eligible for a higher annual update.
CY 2027 is the second year in which, by law, Medicare must implement two separate updates to the Medicare Conversion Factor (CF). A higher 0.75% update applies to clinicians participating in advanced alternative payment models (APMs), while a lower 0.25% update applies to all other clinicians.
While the initial gap between the two CFs is small, as multiple analysts have observed, the cumulative effect of differing annual effects over time is significant. Yet, this could be the point. It incentivizes physicians to participate in value-based care. Stakeholders have noted that many specialties lack value-based care options within Medicare, creating an inherent unfairness in the dual CF structure.
Both CFs will also be affected by budget neutrality. Budget neutrality is a federal rule that requires any policy changes that increase spending by $20 million or more to be offset by equivalent reductions elsewhere. This adjustment is typically made by reducing the CF.
#2: Efficiency Adjustment Part 2.
CMS may seek to further implement the goals of the 2.5% across-the-board cut on work RVUs for non-time-based codes, known as the efficiency adjustment, which was first introduced in 2026..
The efficiency adjustment is part of a broader CMS strategy to prioritize advanced primary care and chronic care management. In the 2027 proposed rule, we may see additional initiatives as the agency continues to advance these goals.
CMS has been very transparent about seeking new data sources for ratesetting beyond those the agency has historically used. In public comments, CMS leadership indicated that the seed for the efficiency adjustment idea came from analyzing anesthesia time in claims data, which appeared to show a decline in procedure time. The agency has also solicited ideas for data sources for ratesetting through the public comment process. CMS may introduce new data sources for ratesetting in the 2027 proposed rule or seek comment on proposed alternative methodologies.
While the efficiency adjustment was supported by certain stakeholders (e.g., many in the primary care community), the agency faced significant pushback from others. There has been discussion that CMS may include a request for public comments in the proposed rule, seeking input on alternative methods for implementing the efficiency adjustment or on related issues.
#3: 2027 Coding Changes.
As a result of increased transparency in the American Medical Association (AMA)/RVS Update Committee (RUC) process, much more is known about CPT code changes and RUC recommendations before the release of the 2027 Medicare PFS Proposed Rule than in previous years.
In a significant policy change, the RUC now publishes meeting minutes, including recommendations submitted to CMS, 30 days after each meeting, rather than after the proposed rule is released. This transition to greater transparency by the RUC provides the general public with more information about the 2027 coding changes and the RUC recommendations submitted to CMS than was previously available.
A February 3, 2026, letter indicates that the RUC submitted recommendations for 153 new/revised/related family CPT codes for the 2027 Medicare PFS. In addition, the RUC submitted 29 recommendations for the potentially misvalued services project.
Maternal health coding changes for 2027 have drawn significant attention. Effective January 1, 2027, the current maternity care global codes will be unbundled. Services will be reported separately by process of care: antepartum visits, labor management, delivery, and postpartum visits. Some have observed that unbundling appears to be a step back from the trend toward value-based care and may create perverse incentives for clinicians. The American College of Obstetricians and Gynecologists and the AMA have said that these changes are appropriate because they better reflect how maternity care is provided today. The stakes are high, with the United States spending over $100 billion annually on maternal care. Stakeholders will closely watch how the agency and commercial payers respond to these changes, as well as to the proposed payment rates and other policies related to the new coding structure.
#4: Proposals that Advance the Trump Administration Priorities.
The administration has been very active in pursuing initiatives across several areas, including tackling fraud, increasing the use of artificial intelligence (AI) across all aspects of the Department of Health and Human Services (HHS), expanding prior authorization (sometimes with AI), and integrating technology into patient care.
Proposals may reflect further advancements of these priorities. CMS is using a range of tools and levers to advance these priorities.
In December 2025, HHS issued a request for information to advance AI in clinical care. Since then, HHS has established the “one HHS” approach to coordinate efforts across agencies.
Other priority areas for the agency that we may see reflected in proposals include chronic care management and diabetes care and management. Over the past year, CMS has expanded access to digital health tools, tech-enabled chronic disease management, and data sharing through various initiatives. We may see additional initiatives in this area in the proposed regulations.
#5: Incentives to Accelerate the Transition of Clinicians and Their Patients into APMs or Other Value-Based Care.
CMS has been aggressively promoting innovation models and other strategic efforts to reduce the agency’s fee-for-service footprint.
CMS has been implementing an aggressive value-based care strategy to shift Traditional Medicare into accountable care relationships. With this goal in mind, CMS has launched and proposed numerous value-based care models, some of which are mandatory.
In addition to seeking cost savings, these models have integrated the agency’s priorities to advance AI use and other technologies.
In 2026, CMS announced the Ambulatory Specialty Model, a mandatory five-year risk model that begins on January 1, 2027, and covers specialist care for beneficiaries with cognitive heart failure or low back pain. Further details on the model’s implementation may be included in the proposed rule.
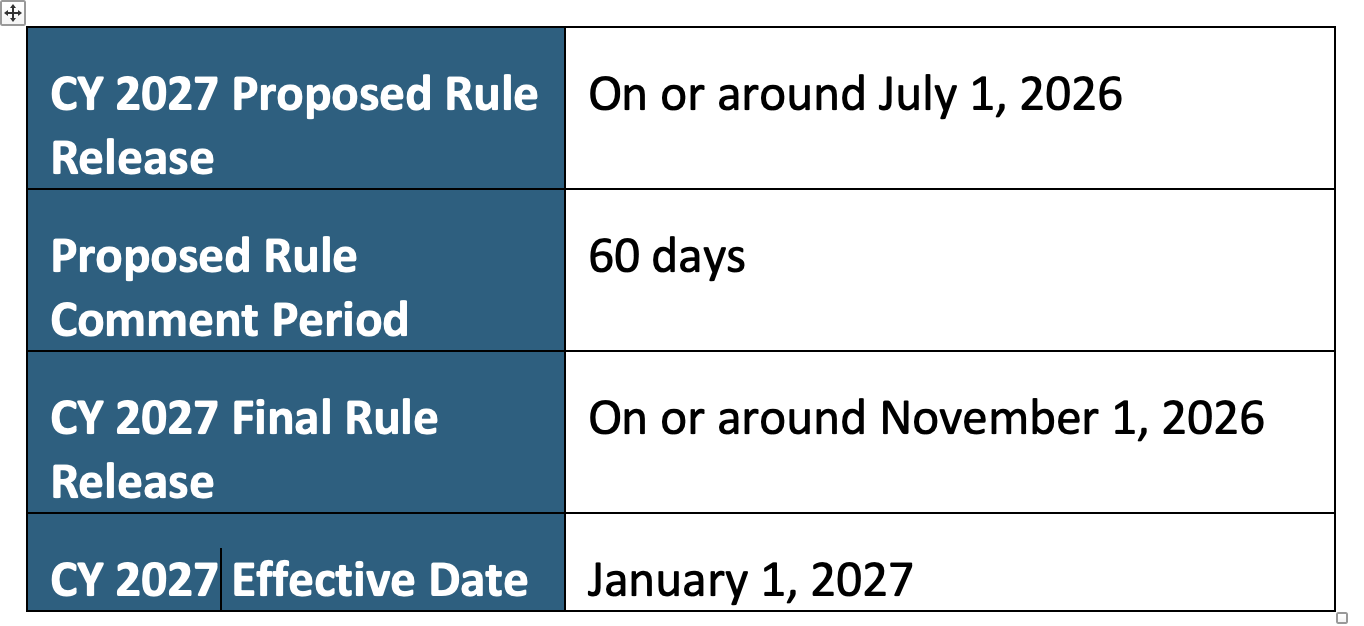
Timeline
The timeline for the CY 2027 Medicare PFS Proposed Rule is below.
Please reach out if you have any questions or would like to discuss the proposed regulations. Further updates and analysis will be posted after the proposed rule is released.
For more information or to discuss, please contact:
Sheila Madhani, MA, MPH
Madhani Healthcare Consulting
smadhani@madhani-health.com/202-679-2977