
States Push Back on E/M Downcoding by Private Insurers
Downcoding is viewed as undermining physician judgment and delaying payment for legitimate care. States are addressing downcoding by private insurers through legislation and fines.
Background: Understanding the Basics of Downcoding
In recent years, clinicians have faced reductions in reimbursement for evaluation and management (E/M) services because of private payors' downcoding practices.
E/M downcoding occurs when insurance payers automatically downgrade a clinician-submitted E/M code to a lower level, resulting in reduced reimbursement.
This often occurs without reviewing medical records; instead, the payor might rely on automated software algorithms or artificial intelligence (AI) to identify high-level codes and pay them as lower-level codes (e.g., 99214 downgraded to 99213), without examining the documentation but based solely on diagnosis codes. It is estimated that insurers began using AI in 2022 to help manage claims.
Downcoding can occur due to the reported diagnosis codes. Physician organizations and other stakeholders argue that selecting the right E/M code should depend not only on the diagnosis code but also on the medical documentation.
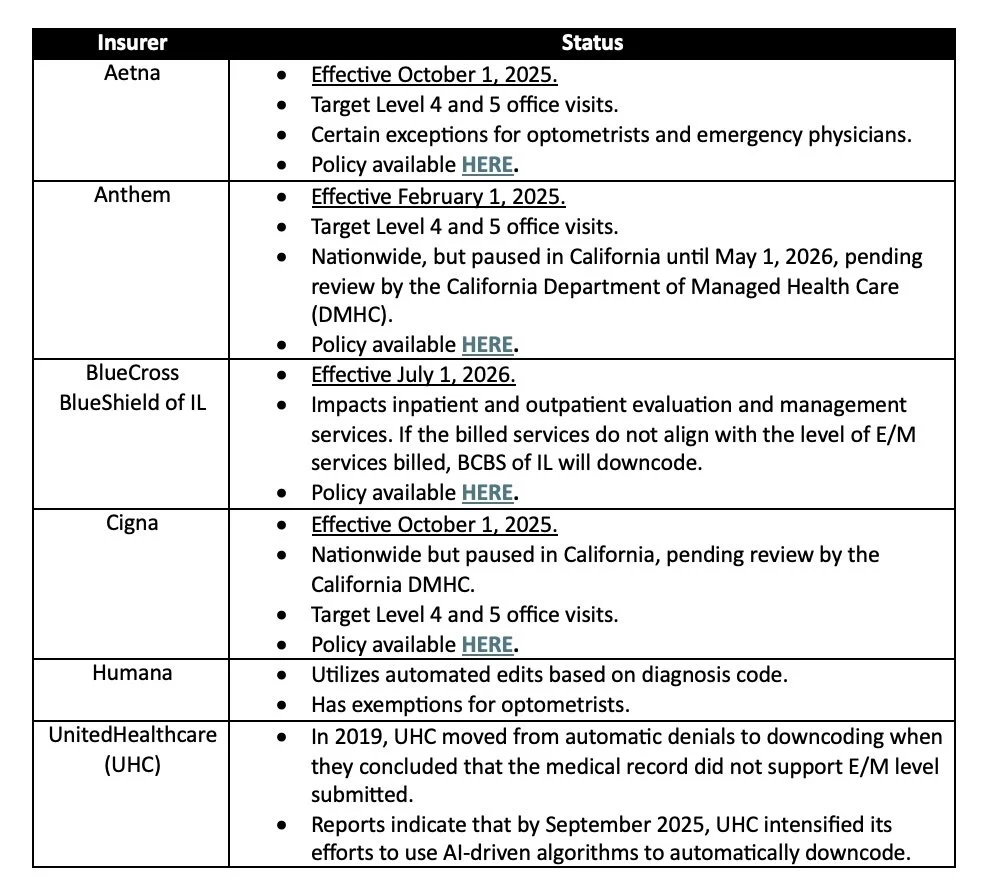
Current Policies
There are numerous examples of private insurers adopting automated downcoding policies for E/M services.
Actions by States to Challenge E/M Downcoding Policies
Several states have taken action to challenge these policies.
The Maryland Insurance Administration issued a letter to Cigna, announcing an $80,000 fine and requiring the insurer to cease automatic downcoding policies.
As of March 2026, the Indiana Governor signed legislation that restricts health plan downcoding of E/M claims. The law requires notification for downcoded claims, bans AI-only downcoding, prevents targeting complex cases, and establishes a clear appeals process.
The California Medical Association (CMA) has successfully paused several downcoding policies pending review by the California DMHC.
Professional medical associations such as the American Optometric Association and the American College of Emergency Physicians have successfully obtained exemptions for their members.
Several states have legislation in development:
Illinois (SB 3114/HB 4735): The "Transparency in Downcoding Act" prohibits AI from being the only reason for downcoding, requires a licensed physician of the same or similar specialty to review claims, and mandates clear, clinical explanations for any changes.
CMA is sponsoring legislation to prohibit automatic downcoding without human clinical review and to restrict "claim-editing" algorithms in California.
The Ohio State Medical Association supports legislation to fully ban insurers from automatically downcoding in Ohio.
Mitigating Impact of E/M Downcoding Policies
Although some limited progress has been made in fighting automated downcoding policies, they still impose significant financial and administrative burdens on medical practices. Medical practices can create policies to lessen their impact.
Some medical practices might not be aware that their claims are being downcoded. Review your claims and communications with payors to spot any potentially downcoded claims.
It's important to regularly test and evaluate to identify the risk of your E/M codes being downcoded. A crucial part is checking if your practice’s E/M reporting aligns with benchmarks set by similar practices.
It is important that your practice adheres to the proper coding and documentation requirements when billing E/M services.
File appeals for individual claims that are reduced.
The AMA recently published a resource to help medical practices identify downcoding policies and guide their strategic responses.
__________________
For more information and questions, please contact:
Sheila Madhani
Madhani Healthcare Consulting
Email: smadhani@madhani-health.com
Tel: (202) 679-2977